The alert comes in at 7 AM on a Tuesday. Billing reports that a batch of claims weren’t submitted overnight. The revenue cycle manager escalates to engineering. Your team pulls up the integration logs — except the integration doesn’t have logs in any useful sense. It has a status column that says “completed.” Everything completed. Nothing got there.
That gap — between “the system said it ran” and “the data actually moved correctly” — is where healthcare data integration actually lives. Not in the vendor slides about interoperability and connected care. In the 7 AM Slack thread where nobody can explain what happened to 400 ADT messages between your EHR and your billing platform.
Most content on “what is data integration in healthcare” stops at the definitional answer, the same gap the broader guide to what data integration actually requires covers: HL7 v2 for clinical messaging, FHIR for modern API exchange, EDI for payer transactions. Your team already knows this. The harder question is why the integration layer in most health-tech organizations is simultaneously load-bearing and invisible — and what it would actually take to own it.
The patchwork problem is structural, not accidental
Healthcare didn’t land in its current integration state because engineering teams made bad decisions. It landed here because the standards evolved in layers across three decades, each one solving a real problem without replacing what came before.
HL7 v2 was practical in the 1990s and remains dominant in clinical messaging because it works across a massive installed base of EHR systems, lab systems, and patient management platforms. FHIR arrived to fix what v2 couldn’t — structured, API-native data exchange with real resource models — and now sits alongside v2 in most production environments rather than replacing it. EDI X12 handles payer-side transactions and operates on its own cadence entirely. DICOM carries imaging data. CDA carries clinical documents. Each layer is maintained by different organizations, versioned on different schedules, and implemented with varying degrees of fidelity by every vendor in the market.
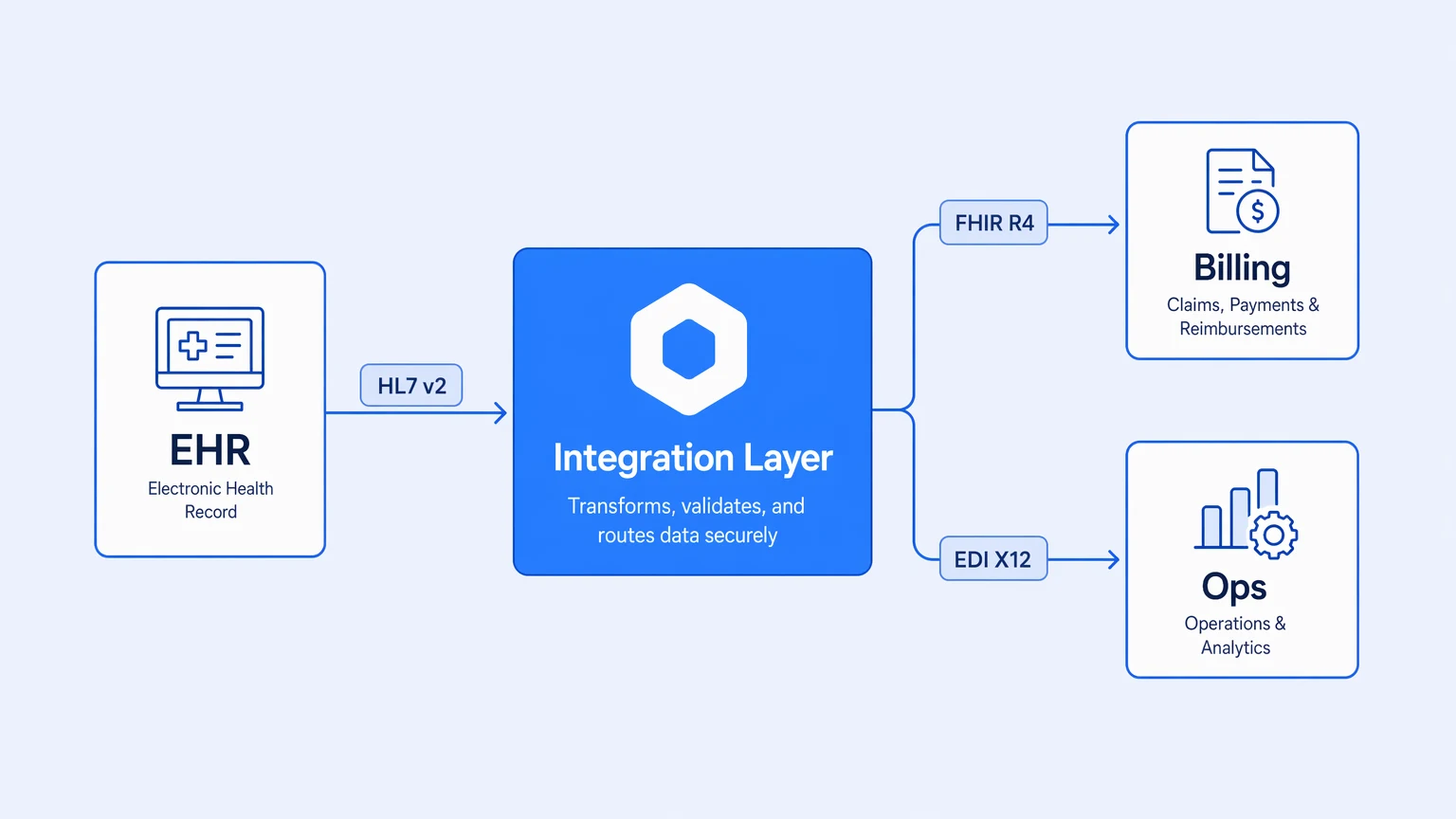
The result is that what we call “healthcare data integration” in 2026 is actually four or five distinct integration problems running simultaneously under the same roof. The EHR talks to clinical systems in HL7 v2. The patient portal exposes FHIR R4 APIs. The billing platform ingests claims via EDI. The ops dashboards pull from a data warehouse that someone fed with a combination of the above plus direct database queries. These aren’t connected by a system — they’re connected by a series of point-to-point integrations, transformation scripts, and middleware configurations that accumulated over years.
Every healthcare engineering team inherits an integration layer that was never designed — it was negotiated.
The fragmentation wouldn’t be fatal if any one piece of it were observable. The actual failure mode isn’t that the systems are different. It’s that when a message drops or transforms incorrectly, the root cause lives in someone’s head, and the fix gets applied to a system nobody fully owns. Finding out took too long. The knowledge that let you fix it doesn’t survive the next team rotation.
Why EHR-to-billing is specifically where things go wrong
Clinical systems and billing systems are built by different vendors, optimized for different users, and operated on different data models. The integration between them is where more revenue-cycle engineering time disappears than almost any other layer.
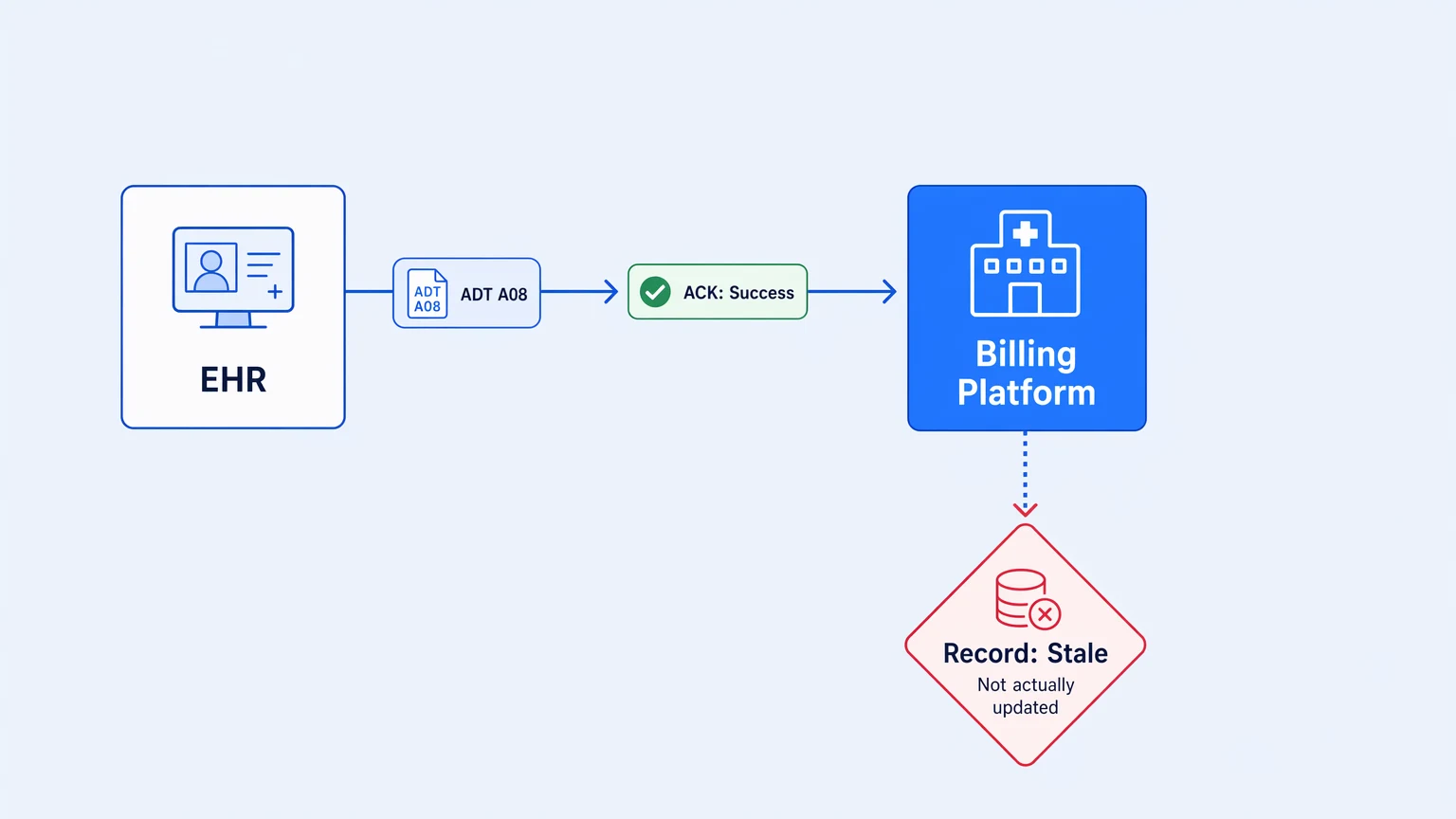
The failure modes are predictable once you’ve seen them. An ADT A08 message updates a patient record in the EHR. The downstream billing system receives the message, sends an ACK, and then silently fails to process the update because the patient identifier didn’t match the expected format. The ACK says success. The billing record stays stale. Nobody notices until the claim is denied.
Or: a FHIR-based patient data API returns a resource successfully, but a field the billing platform requires is only populated when certain clinical flags are set. The integration passes the resource downstream. The billing platform ingests what it can and drops the rest. No error. No alert. A reconciliation report three days later surfaces the discrepancy, and someone has to replay two days of transactions by hand.
These are not edge cases. They are the normal operating condition of a healthcare integration layer that treats the interface contract as “messages arrive” rather than “messages arrive correctly and with the content downstream systems need.”
The standard response is to add monitoring — another dashboard, another alert rule, another reconciliation script. This compounds the original problem. Now you have a fragmented integration layer and a fragmented monitoring layer, and the two disagree in interesting ways at exactly the moments that matter.
The EHR-to-billing integration doesn’t fail loudly. It fails in ways that look like success until someone reconciles a report that nobody reads until end of month.
Ops systems connect last and break first
The integration path from EHR to billing gets the most engineering attention because revenue cycle pain is visible and expensive. Ops systems — scheduling, bed management, capacity analytics, workforce tools — are typically connected later, with fewer resources, and on tighter timelines.
The result is that the ops integration layer often has the thinnest test coverage and the least observability. A scheduling system integration that pushes appointment data to a capacity dashboard might run perfectly for six months and then break silently when the EHR vendor ships a format change to an ADT segment. The capacity dashboard still shows numbers. They’re just wrong — pulled from stale cache or computed on incomplete data — and nobody notices because the numbers didn’t change dramatically enough to trigger an alert.
The failure mode here isn’t a missing message. It’s a transformation that runs without error on malformed input and produces plausible-looking output. This is harder to catch than a delivery failure. Delivery failures show up in exception logs. Silent data quality failures show up in board presentations when someone asks a question and the number doesn’t match what clinical operations remembers.
The ops integration problem isn’t connectivity — it’s confidence that the data flowing through is actually what you think it is.
Fixing this requires something more fundamental than additional monitoring. The integration layer itself needs to be observable at the activity level — not just “did the message arrive” but “what did each transformation produce, what was the input, and does it match what downstream systems received.” That’s a different architecture bar than what most healthcare integration tooling was built to meet.
What production-grade healthcare data integration actually requires
The definitional answer to “what is data integration in healthcare” is the standards catalog above. The production answer is different: it’s the set of properties your integration layer needs before you trust it with patient data, revenue cycle, and ops decisions.
The list is shorter than you’d expect. Most organizations are missing at least two of the three.
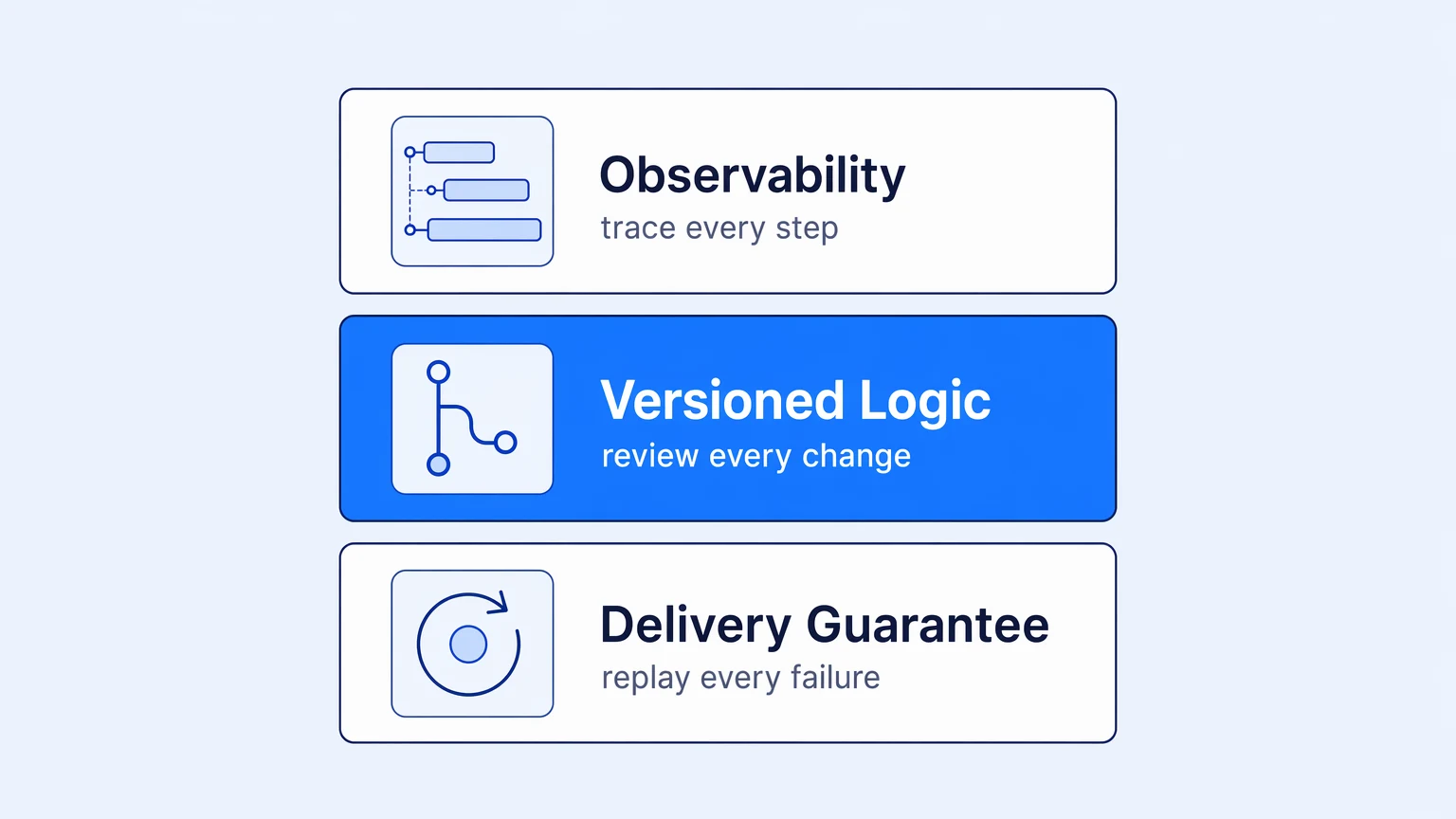
Observability at the message level, not the pipeline level. Knowing that a pipeline ran tells you almost nothing. Distributed tracing on integration workflows — the same kind you’d instrument for a production service — means you can follow a specific patient record through every step from EHR ingest to billing output and see exactly where data changed and whether it changed correctly. This is table stakes for any system that feeds revenue cycle.
Versioned, reviewable integration logic. An HL7 v2 to FHIR transformation rule that lives in a vendor’s drag-and-drop UI is logic that nobody can review, nobody can test in isolation, and nobody can roll back when the vendor ships an update. That’s not a Git preference — it’s a production risk. When a transformation changes in a healthcare context, you need to know when it changed, what changed, and who approved it. The audit trail is as important as the code itself.
A delivery guarantee with replay. Messages that arrive but fail processing should be captured with their full payload and replayable. Not emailed to a DL. Not written to a flat file someone checks monthly. Captured, attributed, alertable, and replayable through the same pipeline with the same trace visibility you’d have on a fresh ingest.
These aren’t aspirational properties. They’re the engineering minimum for a system that touches patient data and drives revenue decisions. Most healthcare organizations are operating below this floor — not because engineering teams don’t know better, but because the tooling they inherited wasn’t built to this bar.
The longer argument on what it means to actually own your integration layer — rather than rent it from a vendor who keeps the logic and the telemetry in their own database — is here, in why unobservable integration stacks are the real hidden bill.
Building toward it
Teams that get this right don’t do it with a single platform migration. They start with the highest-stakes path — usually EHR-to-billing — instrument it properly, build the deployment and rollback workflow, and use that as the template for the next one.
The sequence that works: observability baseline first (you can’t fix what you can’t see), then version-control the transformation logic, then add the delivery guarantee layer. Each step pays off independently. You don’t need all three in place before the first one earns its keep.
When evaluating integration platforms for this work, skip the connector count comparison. The questions that actually matter: what does the platform emit as telemetry, can integration logic live in your repo, and what happens to a message that fails processing. Those three tell you most of what you need to know about whether the platform was built for production or for demos.
Koodisi is built around exactly this model — OpenTelemetry on every tier from the Community plan, real Git versioning with in-platform branching and PRs through your existing GitHub or GitLab flow, and delivery failures captured with one-click replay. No per-execution billing, no overage invoices. Your bill doesn’t move when a FHIR batch job runs larger than expected. Start on the Community tier and trace a real workflow — the observability view alone is worth the fifteen minutes.